
A Clinical Guide to How We See: Image Formation and the Visual Pathway
- David B. Sabin

- 11 hours ago
- 6 min read
The image formation diagram is a useful patient-education tool because it shows the basic optical pathway: light enters the eye, refracts through the cornea and lens, focuses on the retina, and then travels through the optic nerve to the brain.
Clinically, however, “seeing” is more than optics. Vision requires a functioning anterior segment, clear ocular media, accurate refractive focusing, healthy photoreceptors, intact retinal circuitry, organized retinal ganglion cell axons, and preserved post-retinal pathways through the optic nerve, chiasm, optic tract, lateral geniculate nucleus, optic radiations, and primary visual cortex. StatPearls describes the visual pathway as a continuous neuronal system transmitting information from the retina through the optic nerve, optic chiasm, optic tracts, LGN, optic radiations, and ultimately the occipital lobe.

1. Optical Image Formation: Cornea, Pupil, Lens, and Retina
The first stage of vision is optical.
Light from an object enters the eye through the tear film and cornea. The cornea provides the first major refractive surface and begins bending incoming light rays toward a focal point. The pupil then controls the aperture of the system, while the crystalline lens fine-tunes focus.
The diagram correctly shows the cornea and lens refracting light so rays converge on the retina. For a clear retinal image, the optical system must focus light precisely at the photoreceptor plane. If the focal point falls in front of or behind the retina, the patient experiences refractive blur, such as myopia, hyperopia, or astigmatism.
The pupil affects image quality by regulating light entry, depth of focus, and optical aberrations. A smaller pupil increases depth of focus but may reduce retinal illuminance. A larger pupil improves light entry but can increase higher-order aberrations and symptoms such as glare or halos.
The lens provides dynamic focusing through accommodation. With age, decreased lens flexibility reduces accommodative amplitude, producing presbyopia.

2. The Retinal Image Is Real and Inverted
The image formed on the retina is a real, inverted image.
This is an important concept for patients and students. The eye’s optical system focuses light in a way that flips the image vertically and reverses it horizontally at the retinal level. The patient does not perceive the world upside down because the visual cortex interprets the retinal signals in spatial context.
In clinical terms, this inversion matters when interpreting visual fields. The superior visual field projects to the inferior retina, and the inferior visual field projects to the superior retina. Similarly, the temporal visual field projects to the nasal retina, and the nasal visual field projects to the temporal retina.

3. Phototransduction: Converting Light Into Neural Signal
Once light reaches the retina, the process shifts from optics to neurobiology.
The retina contains photoreceptors — rods and cones — that convert photons into electrical signals. These signals are then processed through bipolar, horizontal, and amacrine cells before converging on retinal ganglion cells. Retinal ganglion cell axons form the retinal nerve fiber layer and exit the eye at the optic disc, where the absence of photoreceptors creates the physiologic blind spot.
Clinically:
Rods are more involved in scotopic vision, peripheral detection, and motion sensitivity.
Cones are concentrated in the macula and fovea and are responsible for high-resolution acuity, color vision, and photopic detail.
The macula gives central detailed vision, while the peripheral retina contributes to spatial awareness, motion detection, and peripheral field function.
4. Retinal Ganglion Cells and the Optic Nerve
After retinal processing, visual information exits the eye through retinal ganglion cell axons.
These axons form the optic nerve, which is not simply a passive cable. It is an organized central nervous system white matter tract carrying topographically arranged visual information. StatPearls describes the optic nerve as consisting of approximately 1.2 million retinal ganglion cell axons.
This is clinically important in glaucoma, optic neuritis, ischemic optic neuropathy, compressive optic neuropathy, papilledema, and toxic/nutritional optic neuropathies.
Damage at the retina or optic nerve generally produces monocular defects because the lesion occurs before the optic chiasm. Central scotomas, arcuate defects, nasal steps, enlarged blind spots, and nerve fiber bundle defects can often localize pathology to the retina, macula, optic nerve head, or retinal nerve fiber layer.

5. The Optic Chiasm: Where Fibers Cross
The optic nerves from both eyes meet at the optic chiasm.
At the chiasm, nasal retinal fibers cross to the opposite side, while temporal retinal fibers remain uncrossed. This crossing allows each hemisphere of the brain to receive information from the opposite visual field. StatPearls notes that approximately 53% to 57% of fibers cross at the optic chiasm.
This organization is the foundation of neuro-ophthalmic localization.
A chiasmal lesion classically produces a bitemporal hemianopia because crossing nasal retinal fibers carry temporal visual field information from both eyes. Common causes include compressive lesions near the sella, such as pituitary adenoma, meningioma, craniopharyngioma, aneurysm, or glioma, as summarized by the Merck Manual.
6. Optic Tracts: Contralateral Visual Field Information
Posterior to the chiasm, the fibers are reorganized into the optic tracts.
Each optic tract carries information from the contralateral visual field of both eyes. For example, the right optic tract carries information from the left visual field.
Because post-chiasmal lesions affect information from both eyes, they typically produce homonymous visual field defects. The Merck Manual explains that retrochiasmal lesions produce homonymous defects and that these defects tend to become more congruous with more posterior lesions.
Clinically, this is why a homonymous hemianopia should raise concern for retrochiasmal disease, including stroke, tumor, trauma, demyelination, or other intracranial pathology.
7. Lateral Geniculate Nucleus: The Thalamic Relay
Most optic tract fibers synapse in the lateral geniculate nucleus, or LGN, of the thalamus.
The LGN preserves retinotopic organization and separates functional channels that support motion, form, and color processing. StatPearls describes the LGN as a six-layered gray matter relay that maintains eye-specific and functional segregation, including magnocellular and parvocellular pathways.
From a practical standpoint, LGN lesions are less common than optic nerve, chiasmal, or cortical lesions, but they can produce characteristic homonymous field defects depending on vascular territory and lesion location.

8. Optic Radiations: Temporal and Parietal Pathways
From the LGN, visual signals travel through the optic radiations, also called the geniculocalcarine tract.
The optic radiations split into clinically important pathways:
The inferior fibers, known as Meyer’s loop, travel through the temporal lobe and carry superior visual field information.
The superior fibers travel through the parietal lobe and carry inferior visual field information.
StatPearls describes this arrangement and notes that lesions of these pathways produce predictable homonymous visual field defects.
Clinically:
A temporal lobe lesion affecting Meyer’s loop can produce a contralateral superior quadrantanopia — often remembered as “pie in the sky.”
A parietal lobe lesion can produce a contralateral inferior quadrantanopia — often remembered as “pie on the floor.”
9. Primary Visual Cortex: Conscious Visual Perception
The optic radiations terminate in the primary visual cortex, located along the calcarine fissure of the occipital lobe.
The visual cortex maintains retinotopic organization. The superior bank of the calcarine cortex represents the inferior visual field, while the inferior bank represents the superior visual field. Secondary visual areas then integrate more complex features, including motion, depth, object recognition, spatial awareness, and higher-order visual perception.
This is where the simplified diagram’s final step — “the brain sees the image upright” — becomes clinically meaningful. The brain does not simply flip a picture. It reconstructs visual perception from organized neural signals, combining input from both eyes, comparing contrast and edges, processing motion, assigning spatial location, and integrating memory and recognition.
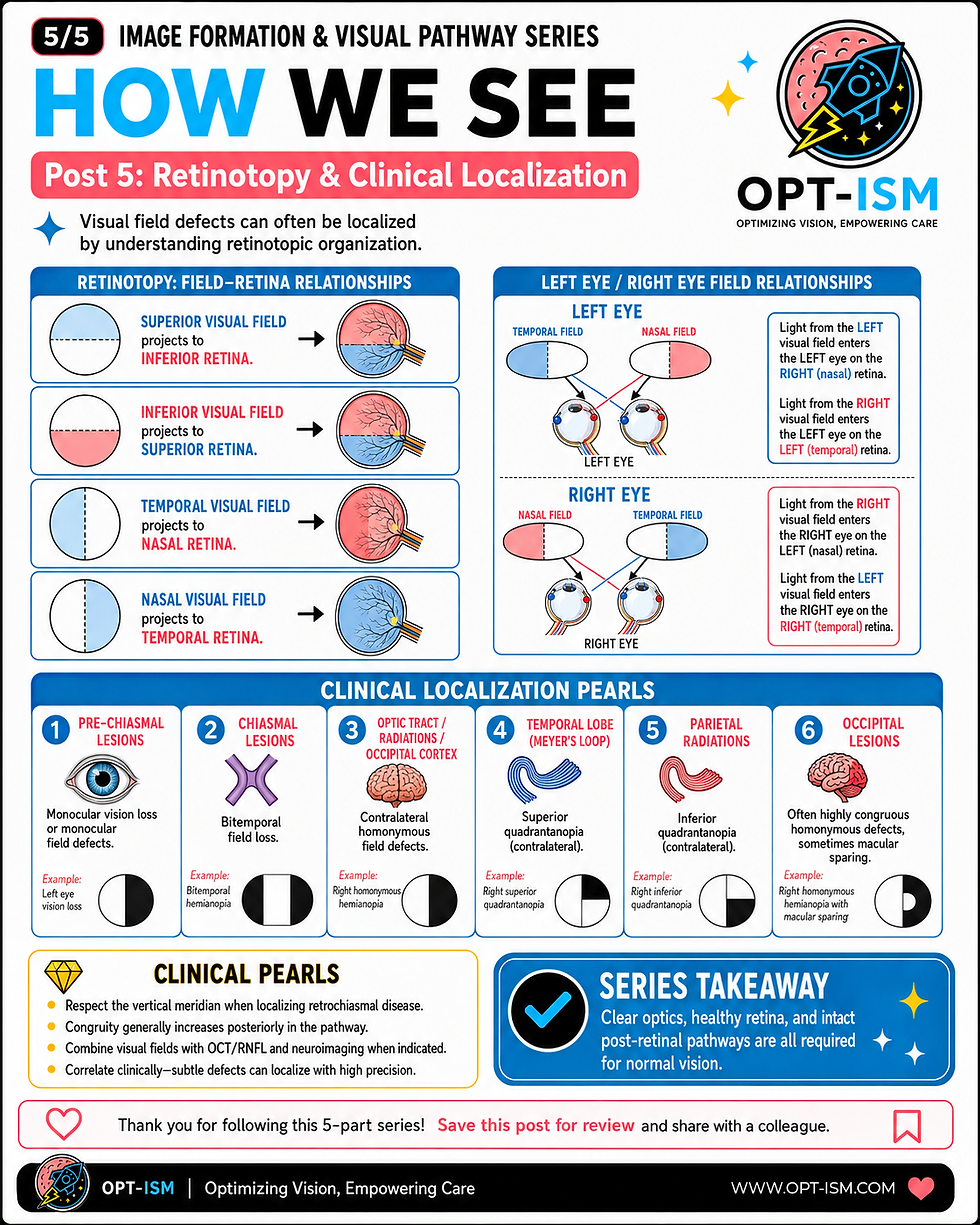
10. Clinical Correlation: Visual Field Defects Localize the Lesion
The visual pathway is organized enough that visual field testing can help localize disease.
A few high-yield localization rules:
Monocular vision loss usually localizes anterior to the chiasm, such as the retina or optic nerve.
Bitemporal hemianopia suggests chiasmal involvement.
Homonymous hemianopia or quadrantanopia suggests post-chiasmal disease.
More congruous homonymous defects often suggest more posterior retrochiasmal lesions.
Arcuate defects, nasal steps, and paracentral scotomas often reflect retinal nerve fiber layer or glaucomatous optic nerve damage.
StatPearls summarizes these localization principles: monocular defects localize anterior to the chiasm, bitemporal defects indicate chiasmal involvement, and homonymous defects reflect postchiasmal pathology.
Clinical Takeaway
The patient version of this image teaches that the eye works like a camera: light enters, focuses, hits the retina, and travels to the brain.
The clinician version is more precise:
The cornea and lens create the retinal image. The retina converts light into neural code. Retinal ganglion cells transmit organized visual information through the optic nerve. The chiasm sorts visual field information. The LGN relays and preserves retinotopy. The optic radiations carry quadrant-specific information. The occipital cortex creates conscious visual perception.
That is why a comprehensive eye exam is not just a refraction. It is an assessment of the entire visual system — from the tear film and cornea to the retina, optic nerve, visual field, and neurologic pathway that allows patients to see the world clearly.



Comments