
Clinical Guide to Color Vision Deficiency: Types, Testing, Medications, and Neurologic Causes
- David B. Sabin

- 20 hours ago
- 12 min read
Color vision deficiency is more than simply being “color blind.” In clinical practice, color vision testing can help identify congenital cone differences, screen for acquired retinal or optic nerve disease, monitor medication toxicity, and document functional vision concerns for school, work, and safety-sensitive occupations.
Most patients described as “color blind” are not completely blind to color. They usually have a partial color vision deficiency, meaning certain hues are harder to distinguish. Complete or near-complete absence of color perception is rare.

Color Deficiency vs. Color Blindness
The term color blindness is commonly used by patients, but it can be misleading. Most affected patients still see color, but they confuse specific color ranges.
A more precise term is color vision deficiency, or CVD.
Color vision deficiency may be:
Congenital, meaning inherited and present from birth.
Acquired, meaning it develops later due to ocular disease, optic nerve disease, neurologic disease, medication toxicity, trauma, or systemic illness.
Congenital red-green color vision deficiency is the most common form and is seen much more often in males because many red-green defects are X-linked.
Basic Clinical Anatomy of Color Vision
Color vision depends on cone photoreceptors in the retina. There are three major cone systems:
L-cones: Long wavelength sensitivity, commonly associated with red perception.
M-cones: Medium wavelength sensitivity, commonly associated with green perception.
S-cones: Short wavelength sensitivity, commonly associated with blue perception.
A color vision deficiency occurs when one cone system is absent, reduced, shifted in sensitivity, or affected by retinal, optic nerve, or neurologic disease. The terms protan, deutan, and tritan refer to abnormalities involving the long-, medium-, and short-wavelength cone systems, respectively.

Major Types of Color Vision Deficiency
1. Protan Defects
A protan defect involves reduced or absent L-cone function.
Clinically, this affects red perception. Patients may report that reds appear darker, less bright, or easier to confuse with black, brown, green, or orange. Protan defects include:
Protanomaly: Abnormal red cone function. The patient still has three cone systems, but red discrimination is reduced.
Protanopia: Absence or nonfunctioning of the red cone pathway. This is more severe than protanomaly.
A key clinical clue with protan defects is reduced brightness perception for red objects.
2. Deutan Defects
A deutan defect involves reduced or absent M-cone function.
This is one of the most common forms of congenital color deficiency. Patients often confuse greens with reds, browns, oranges, and grays.
Deutan defects include:
Deuteranomaly: Abnormal green cone function. This is often milder and common.
Deuteranopia: Absence or nonfunctioning of the green cone pathway.
Compared with protan defects, deutan defects usually do not reduce the perceived brightness of red as much.

3. Tritan Defects
A tritan defect involves reduced or absent S-cone function.
This affects blue-yellow discrimination. Patients may confuse blue with green, yellow with violet, or purple with red. Tritan defects are much less common as inherited conditions but are important clinically because acquired color vision loss often produces blue-yellow changes.
Tritan defects include:
Tritanomaly: Abnormal blue cone function.
Tritanopia: Absence or severe dysfunction of the blue cone pathway.
When a patient develops a new blue-yellow color problem, especially in one eye, consider acquired retinal, optic nerve, lens, or neurologic disease.
4. Achromatopsia
Achromatopsia is rare and much more severe than typical red-green color deficiency. Patients may have severely reduced color perception, light sensitivity, reduced visual acuity, nystagmus, and difficulty in bright environments.
This is not the same as common inherited red-green color deficiency. Achromatopsia is typically a cone dysfunction condition and may require low-vision strategies, tinted lenses, and specialty evaluation.
5. Blue Cone Monochromacy
Blue cone monochromacy is another rare inherited cone disorder. Patients may have reduced visual acuity, photophobia, nystagmus, and severely limited color discrimination. It is clinically different from mild red-green deficiency and may be identified earlier in life due to reduced vision and light sensitivity.

Congenital vs. Acquired Color Vision Deficiency
Congenital Color Vision Deficiency
Congenital color deficiency is usually:
Stable over timeBilateral and relatively symmetricOften red-greenOften discovered in childhood or during occupational screeningNot associated with new pain, vision loss, or neurologic symptoms
Patients may not notice the problem because they have adapted to it since childhood.
Acquired Color Vision Deficiency
Acquired color deficiency deserves more clinical attention. It may be:
New onsetProgressiveAsymmetricWorse in one eyeAssociated with reduced acuity, contrast loss, visual field defects, pain, headache, optic nerve changes, macular disease, or medication exposure
Acquired color vision deficiency can occur from ocular, neurologic, or systemic disease.
A major clinical pearl: new unilateral color desaturation is not “just color blindness” until proven otherwise.

Color Vision Tests and How to Perform Them
Color testing should be performed under controlled conditions. Poor lighting, glare, tinted lenses, dirty plates, faded test books, incorrect viewing distance, and uncorrected near blur can all affect results.
General testing principles:
Test each eye separately when evaluating acquired disease.Use the patient’s best near correction.Use proper illumination, ideally daylight-equivalent lighting.Avoid tinted lenses unless specifically testing real-world function with them.Keep test plates clean and replace faded books.Document the test used, eye tested, number of errors, and pattern of errors.Do not rely on phone or computer “color blind tests” for clinical diagnosis because screen color calibration varies.
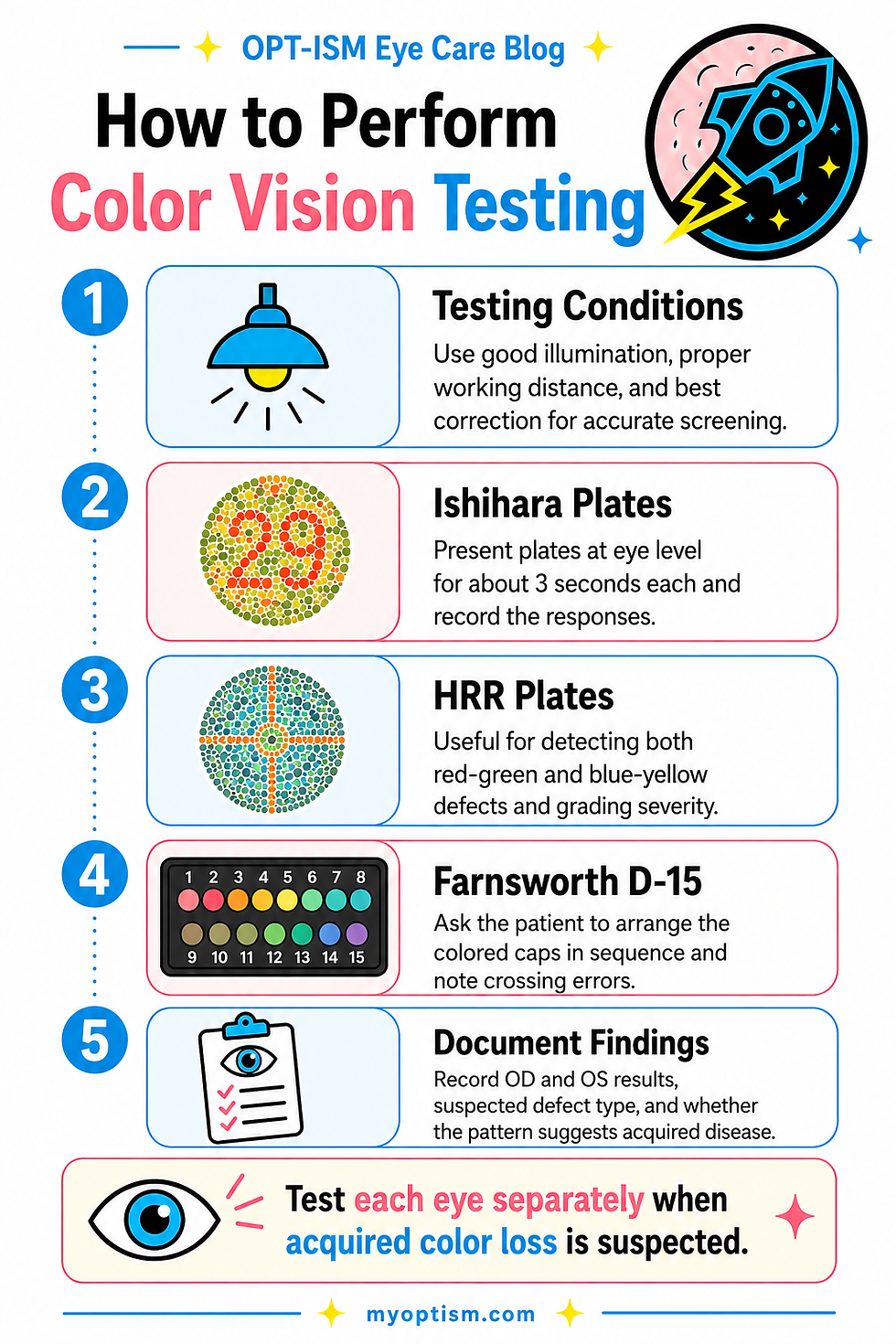
1. Ishihara Color Plates
The Ishihara test is one of the most common clinical screening tests for red-green color deficiency. It uses pseudoisochromatic plates made of colored dots with hidden numbers or pathways. Ishihara is quick and easy, but it is mainly a red-green screening test and has limited ability to fully classify type and severity.
How to Perform Ishihara Testing
Seat the patient comfortably with proper near correction.
Use good standardized lighting. Avoid dim rooms or colored light.
Hold the test at the recommended distance, commonly around reading distance unless the manual states otherwise.
Test one eye at a time if screening for acquired disease. For routine congenital screening, binocular testing is sometimes performed, but monocular testing gives more clinical information.
Show the demonstration plate first to confirm the patient understands the task.
Present each plate for the recommended time, usually only a few seconds. Do not allow prolonged searching.
Ask the patient to identify the number, trace the path, or state that they cannot see it.
Record the number of correct and incorrect responses and note any characteristic red-green error pattern.
Clinical Use
Ishihara is best for detecting congenital red-green deficiency. It is less helpful for blue-yellow defects and may miss some acquired dyschromatopsias.
2. HRR Plates
The Hardy-Rand-Rittler, or HRR, test is another pseudoisochromatic plate test. Unlike Ishihara, HRR can screen for red-green and blue-yellow defects and provides more information about type and severity.
How to Perform HRR Testing
Use proper near correction and standardized lighting.
Test each eye separately if acquired disease is suspected.
Begin with demonstration plates.
Ask the patient to identify symbols or shapes rather than only numbers, which can be helpful for children or patients who do not know numbers.
Proceed through screening plates and then diagnostic/severity plates if errors occur.
Record the error pattern as protan, deutan, tritan, or mixed.
Clinical Use
HRR is useful when you are concerned about acquired dyschromatopsia, optic neuropathy, retinal disease, or blue-yellow defects. Some studies suggest HRR may be more useful than Ishihara for detecting acquired dyschromatopsia from optic neuropathy.
3. Farnsworth D-15 Test
The Farnsworth D-15 is an arrangement test. The patient arranges colored caps in order by hue. It is useful for identifying moderate to severe color vision defects and for differentiating protan, deutan, and tritan confusion axes.
How to Perform Farnsworth D-15 Testing
Use the correct light source and avoid glare.
Place the reference cap first.
Mix the remaining caps in random order.
Ask the patient to arrange the caps in the order that appears to make the smoothest color transition.
Do not coach the patient based on correctness.
After completion, record the cap sequence.
Plot the results on the scoring sheet.
Interpret the pattern of crossing lines to determine whether the errors follow a protan, deutan, or tritan axis.
Clinical Use
The D-15 is helpful when a plate test is failed and you want more information about the type of defect. It can miss mild congenital defects, but it is useful for clinically meaningful deficiencies and for acquired cases when errors are more pronounced. Arrangement tests such as D-15 and Lanthony desaturated D-15 are frequently discussed as useful tools for congenital and acquired color vision assessment.
4. Lanthony Desaturated D-15
The Lanthony desaturated D-15 is similar to the Farnsworth D-15 but uses lower-saturation caps, making it more sensitive for subtle acquired defects.
How to Perform It
The procedure is similar to the Farnsworth D-15:
Use standardized lighting.
Randomize caps.
Have the patient arrange them in hue order.
Record the sequence.
Plot and interpret the error axis.
Clinical Use
This test is helpful when subtle acquired color vision loss is suspected, such as early optic nerve disease, retinal disease, medication toxicity, or mild macular dysfunction.
5. Farnsworth-Munsell 100 Hue Test
The Farnsworth-Munsell 100 Hue test is a more detailed arrangement test. It uses many caps and provides a more refined score for color discrimination.
How to Perform It
Use standardized lighting and the correct viewing distance.
The test is divided into trays of colored caps.
Each tray has fixed end caps.
The patient arranges the movable caps in the smoothest color order between the two end caps.
Score the sequence according to the test instructions.
Analyze total error score and the pattern of errors.
Clinical Use
This test is more time-consuming but can be useful for detailed occupational testing, research, subtle acquired color loss, or monitoring progression.
6. Anomaloscope
The anomaloscope is considered one of the most precise instruments for diagnosing and classifying red-green color vision defects. It requires the patient to match colors by adjusting mixtures of red and green light to match a yellow reference.
How to Perform It
The patient views a split field.
One side contains a reference yellow.
The other side contains a red-green mixture that the patient adjusts.
The patient changes the mixture and brightness until both halves appear to match.
The examiner records the matching range and midpoint.
Clinical Use
The anomaloscope can differentiate protan from deutan defects and distinguish anomalous trichromacy from dichromacy. It is more common in specialty, research, or occupational settings than in routine primary eye care.
7. Red Desaturation Testing
Red desaturation is not a full color vision test, but it is clinically useful when evaluating optic nerve disease.
How to Perform Red Desaturation
Use a bright red target, such as a red bottle cap or red pen tip.
Test one eye at a time.
Ask the patient to compare the brightness and saturation of red between the two eyes.
Ask: “Does the red look equally bright in both eyes, or does it look darker, faded, orange, pink, or washed out in one eye?”
Have the patient grade the difference if possible, such as “the right eye sees red at 60% brightness compared with the left.”
Clinical Use
Red desaturation is commonly used when evaluating optic neuritis, compressive optic neuropathy, ischemic optic neuropathy, asymmetric glaucoma, and other optic nerve disorders.

Medications That Can Cause Color Vision Problems
Medication-related color vision changes are clinically important because they may be reversible if detected early, depending on the medication and severity of toxicity.
Ethambutol
Ethambutol, used for tuberculosis treatment, is a classic medication associated with optic neuropathy. It can cause reduced visual acuity, central or cecocentral scotomas, decreased contrast sensitivity, and color vision loss.
Color vision testing, visual acuity, pupils, optic nerve evaluation, OCT, and visual field testing may be used to monitor suspected toxicity.
Hydroxychloroquine and Chloroquine
Hydroxychloroquine and chloroquine can cause retinal toxicity, classically involving the macula. While modern screening focuses heavily on OCT, automated visual fields, fundus autofluorescence, and sometimes multifocal ERG, color vision complaints may occur in patients with macular dysfunction.
Color changes alone are not enough to diagnose Plaquenil toxicity, but they should prompt careful macular evaluation if symptoms are new.
Digoxin
Digoxin toxicity can cause visual symptoms, classically including yellow-green visual disturbances, halos, blurred vision, and altered color perception. New color complaints in a patient taking digoxin should raise concern for medication toxicity, especially if accompanied by systemic symptoms.
Sildenafil and Other PDE-5 Inhibitors
Sildenafil and related medications can cause transient blue-tinted vision or altered color perception in some patients. This is usually temporary, but persistent or asymmetric symptoms should be evaluated.
Amiodarone
Amiodarone is more commonly associated with corneal verticillata and optic neuropathy concerns. If a patient on amiodarone reports new dyschromatopsia, decreased vision, or visual field symptoms, optic nerve evaluation is appropriate.
Other Medication and Toxicity Considerations
Color vision changes have also been reported with various toxic, nutritional, or medication-related optic neuropathies. When a patient has new acquired dyschromatopsia, review:
Current and recent medicationsDose and durationRenal or liver disease affecting drug clearanceAlcohol useNutritional deficiency riskOccupational or chemical exposureHistory of chemotherapy or antimicrobial use
Medication-associated acquired dyschromatopsia is an important clinical category and has been reviewed in the medical literature.

Neurologic and Optic Nerve Causes of Color Vision Problems
Color vision is often affected in optic nerve disease because the optic nerve carries visual information from the eye to the brain. Color desaturation, especially red desaturation, may be an early clue.
Optic Neuritis
Optic neuritis often presents with decreased vision, pain with eye movement, reduced color saturation, decreased contrast, and an RAPD if unilateral or asymmetric. Patients may say red looks faded, orange, brown, or washed out in one eye.
Color vision testing should be performed monocularly, and results should be compared between eyes.
Multiple Sclerosis
Optic neuritis may be associated with multiple sclerosis. A patient with new unilateral color desaturation, eye pain, and vision loss may need urgent evaluation and possible neuroimaging depending on the clinical picture.
Compressive Optic Neuropathy
Tumors, aneurysms, thyroid eye disease, orbital masses, and other compressive lesions can affect the optic nerve. These patients may show decreased color vision, visual field defects, optic nerve pallor, reduced acuity, or an RAPD.
Slowly progressive unilateral color loss should not be dismissed.
Ischemic Optic Neuropathy
Anterior ischemic optic neuropathy can affect color vision, especially when visual acuity is reduced. Clinically, evaluate optic nerve edema or pallor, visual fields, pupils, vascular risk factors, and symptoms concerning for giant cell arteritis in older patients.
Papilledema and Intracranial Pressure
Papilledema may affect visual function over time. Color vision can be normal early but may become abnormal with optic nerve dysfunction. Evaluate optic nerve appearance, visual fields, OCT RNFL/GCC, symptoms of increased intracranial pressure, and neurologic red flags.
Stroke and Brain Lesions
Color perception can be affected by lesions involving visual processing pathways, including occipital and ventral temporal regions. Patients may describe difficulty naming colors, recognizing colors, or perceiving color normally despite relatively preserved acuity.
Neurologic causes should be considered when symptoms are sudden, associated with visual field loss, weakness, speech difficulty, confusion, severe headache, or other neurologic signs.
Migraine and Transient Neurologic Symptoms
Migraine aura may temporarily alter visual perception, including shimmering, colored lights, scotomas, or visual distortion. Persistent color vision change after a migraine-like episode should be evaluated rather than assumed to be benign.
Ocular Causes of Acquired Color Vision Deficiency
Acquired color vision loss may also come from ocular disease.
Macular Disease
Macular conditions can affect color discrimination because cones are densely concentrated in the macula. Consider color testing in patients with:
Age-related macular degenerationDiabetic macular edemaCentral serous chorioretinopathyMacular dystrophyEpiretinal membraneMacular holePlaquenil toxicity
Glaucoma
Glaucoma is classically associated with optic nerve damage and visual field loss, but color vision and contrast sensitivity may also be affected, especially in more advanced disease. Blue-yellow defects have been discussed in association with acquired optic nerve and retinal disease patterns.
Cataracts and Lens Changes
The crystalline lens yellows with age and can reduce transmission of shorter wavelengths, affecting blue perception. Cataracts may make colors look dull, faded, yellowed, or less vibrant. Patients often report brighter whites and more vivid colors after cataract surgery.
Retinal or Optic Nerve Toxicity
Drug toxicity, nutritional deficiency, alcohol-related optic neuropathy, and toxic exposures can affect color vision. These cases often require careful history, medication review, OCT, visual fields, and coordination with the prescribing physician.
Clinical Workup for New Color Vision Changes
For a patient with new color vision symptoms, consider a more complete workup than a simple Ishihara screen.
History
Ask:
When did the color change start?Is it one eye or both eyes?Is it constant or intermittent?Are colors faded, darker, washed out, yellowed, blue-tinted, or distorted?Any eye pain, especially with eye movement?Any headache, neurologic symptoms, weakness, numbness, or speech changes?Any new medications or dose changes?Any history of TB treatment, Plaquenil use, digoxin, PDE-5 inhibitors, chemotherapy, or toxic exposure?Any occupational color demands?Any family history of color deficiency?Was it noticed since childhood or is it new?
Exam
Include:
Best-corrected visual acuityPupils and RAPD assessmentColor testing monocularlyRed desaturation comparisonContrast sensitivity if availableDilated retinal examMacular evaluationOptic nerve evaluationOCT maculaOCT RNFL/GCCAutomated visual field testing when indicatedMedication reviewNeurologic screening when symptoms warrant
Documentation Tips
Document color vision findings clearly:
“Color vision tested with Ishihara, OD 14/14, OS 8/14.”
“HRR showed tritan-type errors OS greater than OD.”
“Red desaturation: patient reports red cap appears 50% less saturated OD compared with OS.”
“Farnsworth D-15 showed a deutan confusion axis.”
“New unilateral dyschromatopsia with decreased acuity and RAPD; optic nerve workup initiated.”
Good documentation matters for monitoring, referrals, occupational forms, and distinguishing congenital from acquired changes.
Patient Counseling
For congenital color deficiency, explain that the condition is usually stable and not a disease. Patients may benefit from labels, apps, high-contrast cues, occupational counseling, and school accommodations.
For acquired color vision changes, explain that new color changes may be a symptom of retina, optic nerve, medication, or neurologic disease. A comprehensive eye exam helps determine whether the issue is longstanding and benign or new and medically important.
Clinical Takeaway
Color vision testing is simple, but the interpretation can be clinically meaningful.
Ishihara is fast and useful for red-green screening.HRR helps detect red-green and blue-yellow defects.Farnsworth D-15 helps classify moderate defects by confusion axis.Lanthony D-15 is more sensitive for subtle acquired changes.Farnsworth-Munsell 100 Hue provides detailed discrimination scoring.Anomaloscope is the most precise for classifying red-green defects.Red desaturation is a quick optic nerve screening comparison.
The most important clinical distinction is whether the color vision difference is lifelong and symmetric or new, progressive, unilateral, or associated with other visual or neurologic symptoms.


Comments